Effekt av Saphnelo i kliniska studier
Säkerhet och effekt för Saphnelo utvärderades i två 52 veckor långa, randomiserade, dubbelblinda, placebokontrollerade fas III multicenterstudier (TULIP 1 och TULIP 2)19, 28.
Patienterna diagnostiserades med SLE enligt klassifikationskriterierna fastställda av American College of Rheumatology (ACR) från 1997.
TULIP 1 (n = 457) och TULIP 2 (n = 362) var liknande avseende studiernas utformning.
I TULIP 128 var det primära effektmåttet SLE Responder Index (SRI 4)-respons.
I TULIP 219 var det primära effektmåttet British Isles Lupus Assessment Group based Composite Lupus Assessment (BICLA)-respons vid vecka 52.
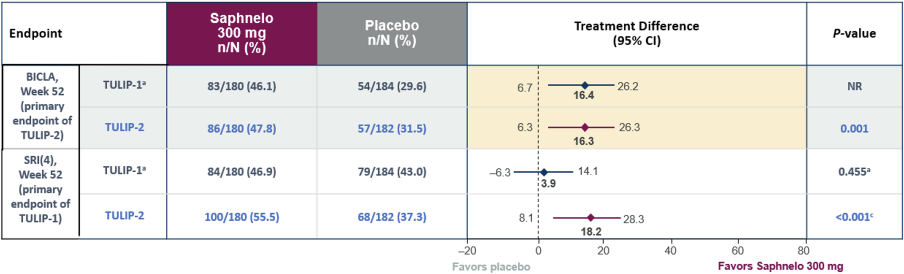
Figuren utvecklad av AstraZeneca baserad på data från referenserna 19 och 28
a The primary endpoint of TULIP-1, SRI-4 response at Week 52, was not statistically significant. Data shown are from the amended rules for restricted medications analysis, which corrected for inappropriately classified NSAID use early in the trial. Therefore, the presented P-value is nominal.
cP-value not adjusted for multiplicity.
Långtids förlängningsstudie (LTE)
En randomiserad, placebokontrollerad, dubbelblindad fas 3 förlängningsstudie (LTE) inkluderade patienter som slutfört TULIP 1 eller TULIP 2. Primärt utfall var långtidssäkerhet och tolerabilitet. Som sekundära explorativa utfall utvärderades ett antal effektmått. I LTE-studien fortsatte patienterna med SAPHNELO 300 mg, eller switchades från SAPNHELO 150 mg till 300 mg, eller re-randomiserades från placebo till antingen SAPHNELO 300 mg eller att fortsätta med placebo22.
1. SAPHNELO associerades med minskad sjukdomsaktivetet och lägre underhållsdos av OCS, jämfört med placebo
Medelvärde av SLEDAI-2K och medelvärde av GC-dos för SAPHNELO + ST eller placebo + ST, per år22
Analysen är beskrivande enbart
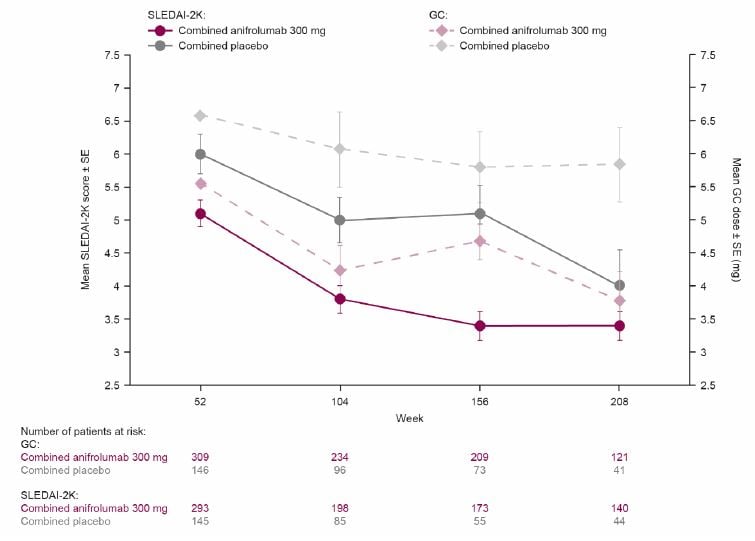
GC, glukokortikoid, SE, standardfel, SLEDAI-2K Systemisk lupus erythematosus sjukdomsaktivitetsindex 2000.
Notera: Analysen exkluderade patienter med glukokortikoiddoser >40 mg/ dag vid baslinjen
2. Remission* från baslinjen till vecka 20824
TULIP-LTE – post hoc analys, deskriptiva data enbart
SAPHNELO associerades med en högre DORIS-remissionsgrad, jämfört med placebo-gruppen24
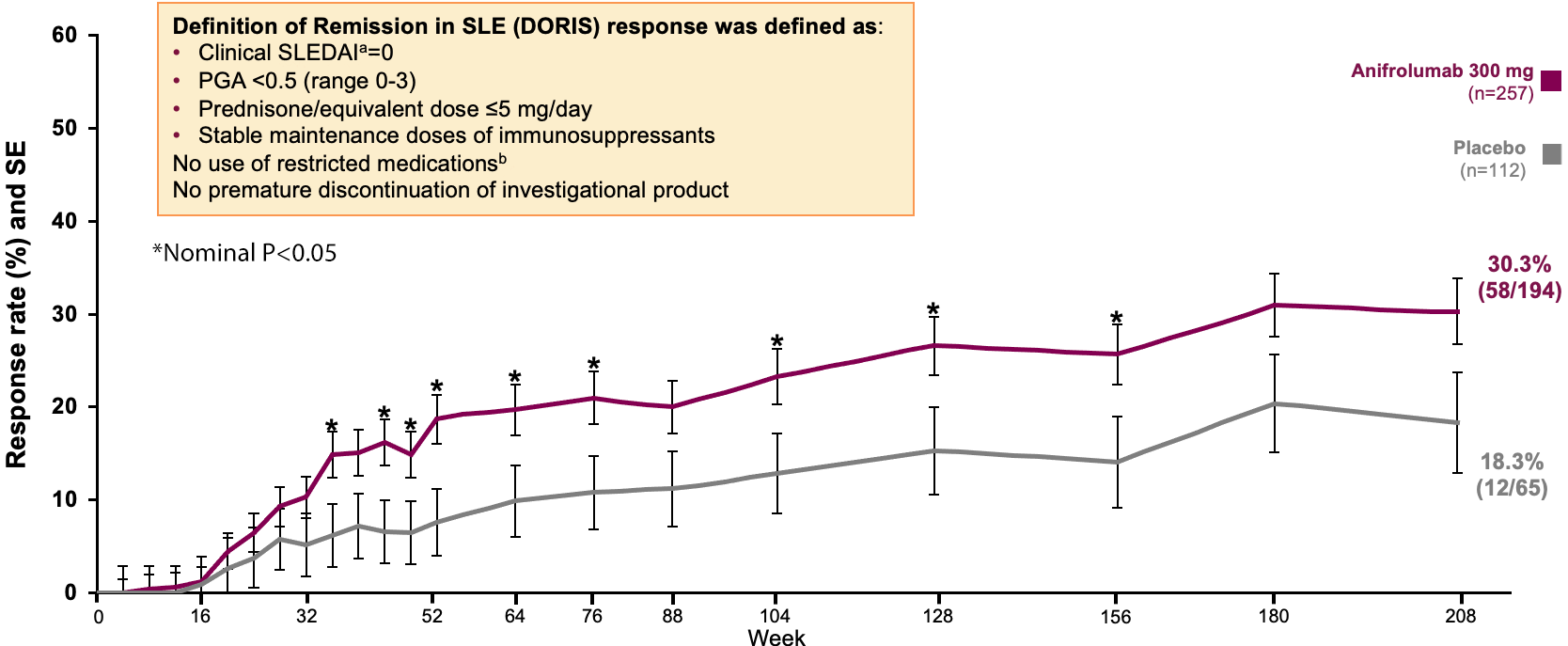
Denna graf utvecklad av AstraZeneca baserad på data från referens 24
aClinical SLEDAI is defined as the sum of all SLEDAI-2K items except increased anti-dsDNA and low complement; b Results for the TULIP-1 and TULIP-2 trial periods utilized the TULIP-2 rules for restricted medications. Restricted medications were not defined during the TULIP LTE period. Stable immunosuppressants were only assessed during the LTE period.
*Remission is defined by: Clinical SLEDAI-2K (sum of all SLEDAI-2K items except increased DNA binding and low complement) = 0, PGA<0.5, prednisone or equivalent dosage≤5 mg/day, and stable doses of immunosuppressants; antimalarials were permitted.’ DORIS attainment was assigned only if patients had no breach of concomitant medication rules and had not discontinued investigational product. No use of restricted medications (TULIP-1/TULIP-2 periods only) and no premature discontinuation of investigational product was allowed. Clinical SLEDAI is defined as the sum of all SLEDAI-2K items except increased anti-dsDNA and low complement.
3. Förmåga att uppnå LLDAS† över 4 år av behandling25
TULIP-LTE - post-hoc analys*, deskriptiva data enbart
SAPHNELO associerades med tidigare uppnådd LLDAS samt mer kumulativ spenderad tid i LLDAS jämfört med placebo-gruppen25
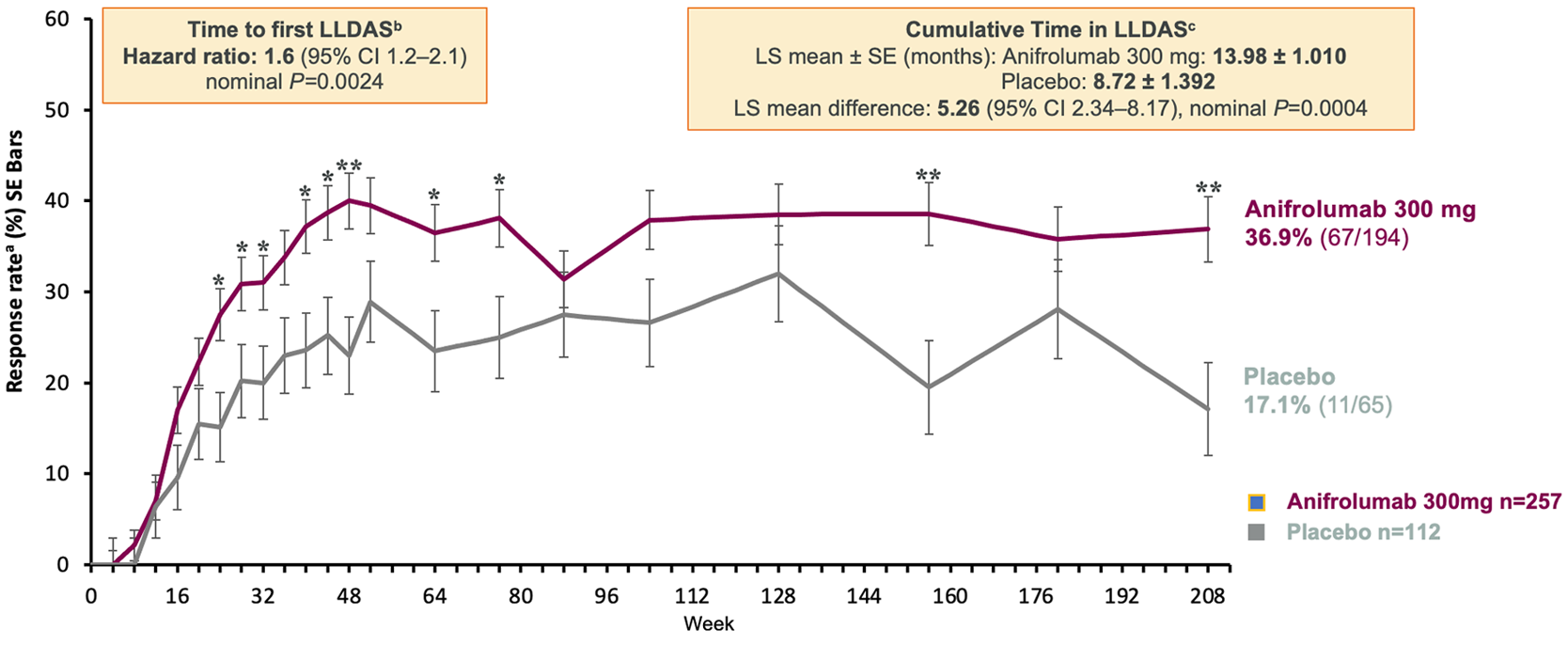
Denna graf utvecklad av AstraZeneca baserad på data från referens 25
*Poolade data analyserade från TULIP-baslinjen till slutet av LTE (vecka 208) för patienter som tilldelades och fick samma studieläkemedel under TULIP+LTE-perioderna (anifrolumab 300 mg eller placebo).
aResponder rates were calculated using a stratified CMH approach, with the same stratification factors as for the Cox regression; odds ratios, 95% CIs, and nominal P-values were calculated using logistic regression with the same stratification factors as for the Cox regression.
bHazard ratio, 95% CI, and nominal P-value was calculated using a Cox regression with the same factors as for the CMH approach.
cAnalyses were calculated using ANCOVA, with stratification factors of SLEDAI-2K at screening, glucocorticoid dosage at Day 1, type I IFN gene signature at screening, and study. Cumulative time spent in LLDAS is the sum of all the time spent in LLDAS. Time spent in LLDAS is calculated as the number of days between a visit with attained LLDAS and the corresponding succeeding visit (with Week 208 as the upper limit), or discontinuation of IP, whichever comes first. *Nominal P<0.05, **Nominal P<0.01.
†LLDAS is defined as: SLEDAI-2K ≤4, with no activity in major organ systems (renal, CNS, cardiopulmonary, vasculitis and fever) and no haemolytic anaemia or gastrointestinal activity, no new features of lupus disease activity compared with the previous assessment, SELENA-SLEDAI PGA ≤1 (0-3), current prednisone (or equivalent) dose ≤7.5 mg daily, and well-tolerated standard maintenance doses of immunosuppressive drugs and approved biological agents, excluding investigational drugs. All components are required simultaneously for LLDAS to be achieved.